HOME - BLOOD - EQUIPMENT - ANATOMY - COMPLICATIONS - PREPARATION - VIDEOS - COURSE CLOSURE
Anatomy: Finding, manipulating, and choosing veins!














Can you spot any anatomy and physiology pointers that could benefit a phlebotomist to know about?
PALPATION TAKES TIME
What are you trying to find?
The right structure (VEINS!)
The direction: feel whole vein. Start puncture at beginning allowing room to insert needle. Consider the depth and angle needed to penetrate
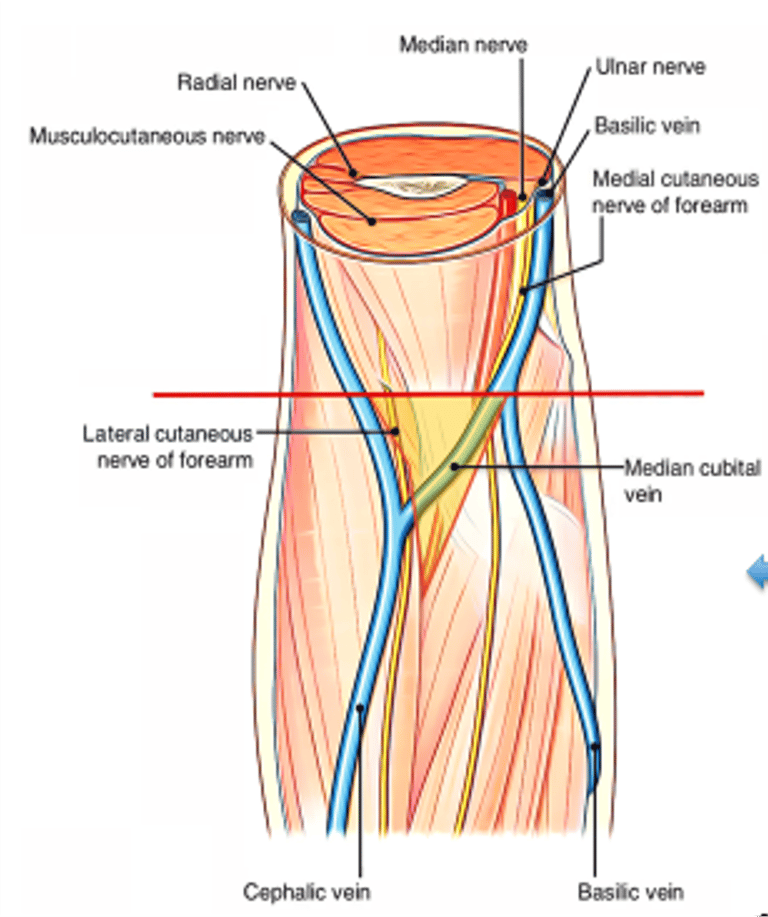
The best option: Always try for median cubital first so CHECK BOTH SIDES even if there is a prominent cephalic/basillic.
The size and stability of the vein
The back up attempt
FEEL FEEL FEEL
Only choose another site to ACF if confident and experienced
Positioning and Location
What are you trying to avoid?
Avoid collecting in same side of running IV infusion
Avoid injecting where veins intersect. (Hematoma risk)
Do not take from varicose veins, fistulas or puncture through damaged tissue
Do not take from same side as CVA, mastectomy, or lymph gland removal (without medical authorisation)
Enter at <30 degree angle MAXIMUM to avoid other structures
DO come in and out at the same angle
DO use correct order of anatomical preference
ALWAYS search BOTH ACF’s first for the safest possible area
DO hold needle steady and anchor it
DO NOT go in at more than 30 degree angle, keep needle angle shallow
DO NOT dig or probe
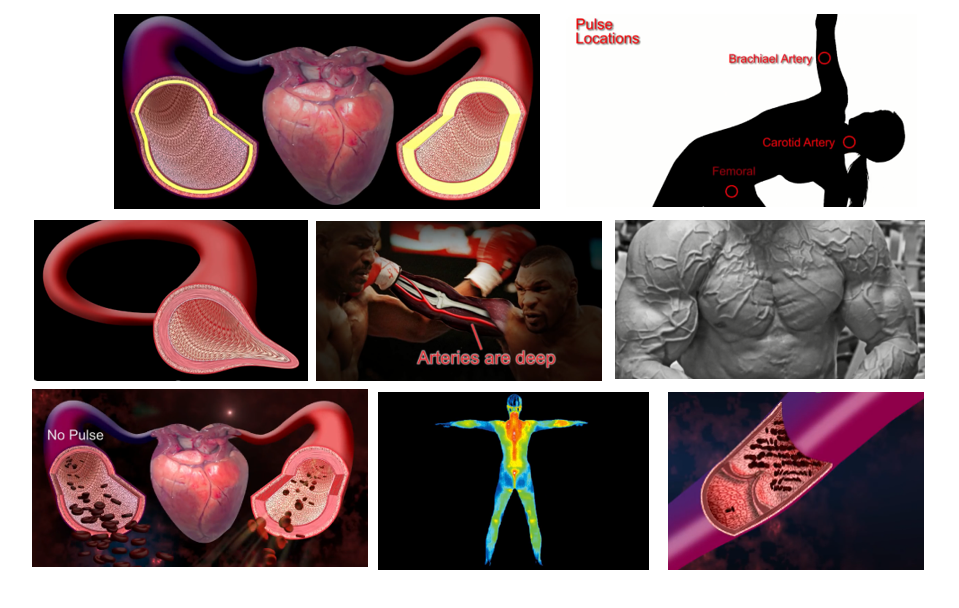
WITHDRAW NEEDLE IMMEDIATELY if excessive or shooting pain, twitching, or pulsating bleeding is observed
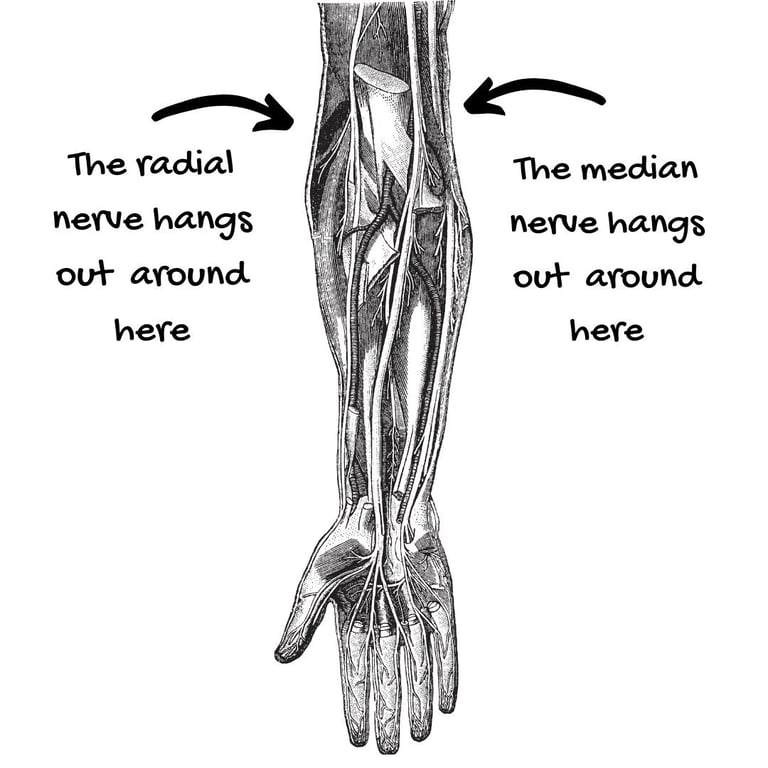
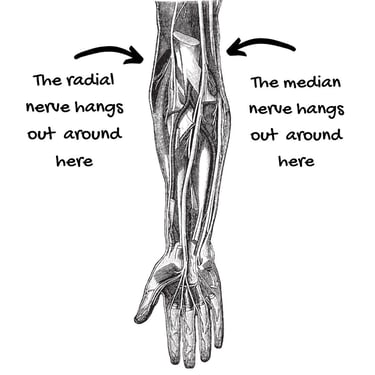
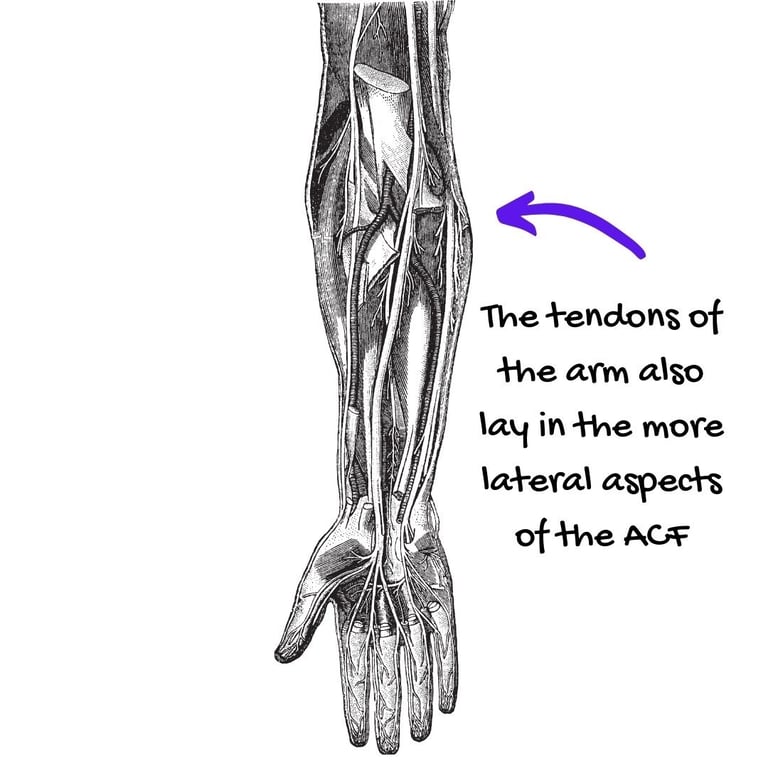
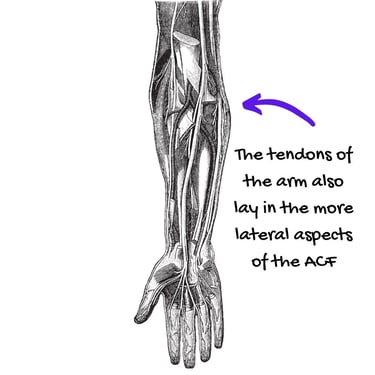
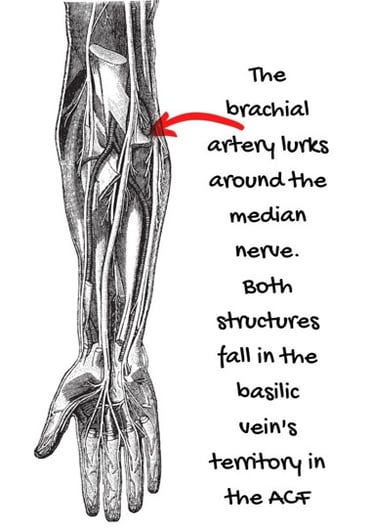
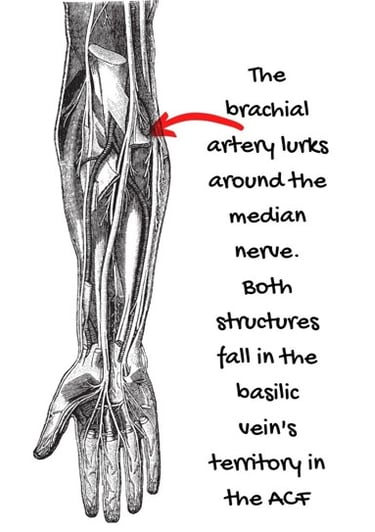
Things you don't want to stab!!
Knowledge check:
Which vein would be your first choice here?
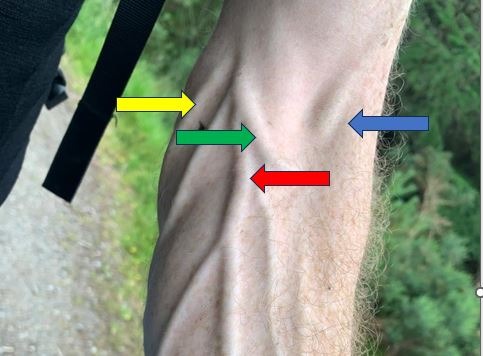
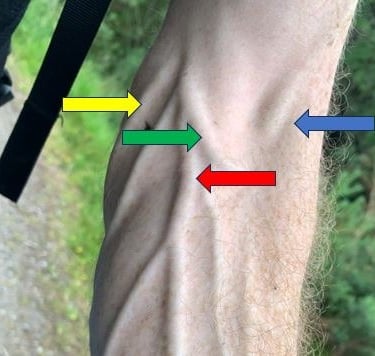
Which of your OWN veins would be your first choice?
Tourniquet Skills! One of your most important tools.
Your aim is to pool the blood
FIGHT GRAVITY: Angle arm down
Don’t be shy on tension if required
TIMING: Allow blood to pool (and drain)
Position near to site (3-4 finger widths)
Hyperextend arm – use cushion
Wiggle fingers initially
Make fist BUT don’t pump fist
Don’t ‘slap’ veins
Re-position as required
What’s the wrist doing?
Watch out for dangly bits!
Ensure a ‘quick release’ tie- no knots!
Single use or wipeable only! A study by Leitch et al (2006) showed that 25% of non-disposable tourniquets were contaminated with MRSA




Get lots of practice!
HOME - BLOOD - EQUIPMENT - ANATOMY - COMPLICATIONS - PREPARATION - VIDEOS - COURSE CLOSURE