If you are looking at this as part of a wider course, please choose the right course to return to! (you will need to re-enter the password given out on the course)

Influenza & COVID-19


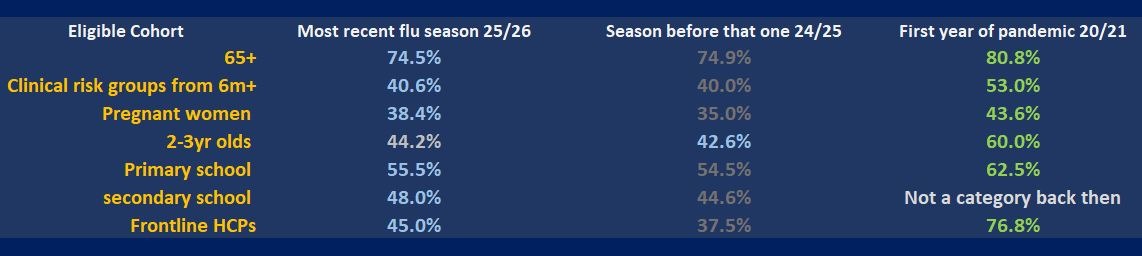
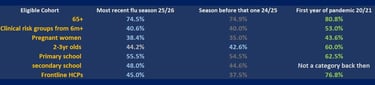
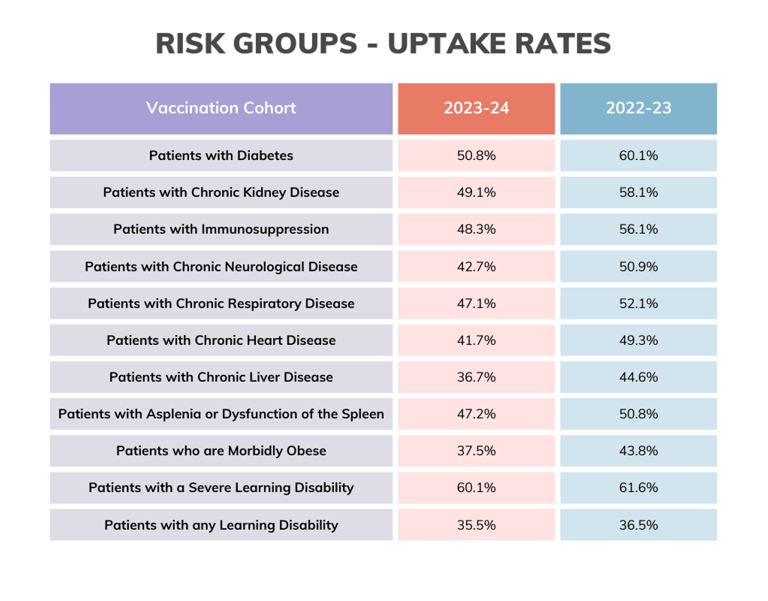
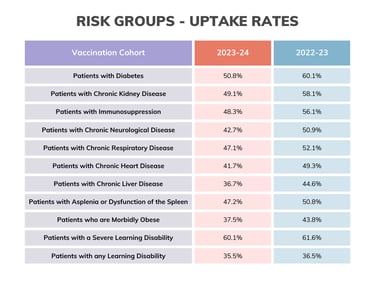
The above vaccine uptake data is concerning seeing as UKHSA published modelling estimates which suggested that flu vaccination had prevented approximately 100,000 hospitalisations in the 24/25 season in England. And more recent modelling indicated that, in England, the 25/26 vaccination programme prevented an estimated 104,000 hospital admissions and 7,100 deaths.
Sadly, we hit the 25/26 flu season five weeks earlier than usual. Australia experienced a severe winter; France and Japan also reported very high activity. There was a mutated A strain in the summer which is always a risk when deciding on vaccine strains so far in advance. Hence, 25/26 was a VERY challenging season.
Antigenic shift and drift can be a real problem (see video below).... Fortunately the 25/26 vaccines maintained their effectiveness. PHEW!
Influenza
Every year we eagerly await the 'flu letter' so we know what we are doing in the coming season.
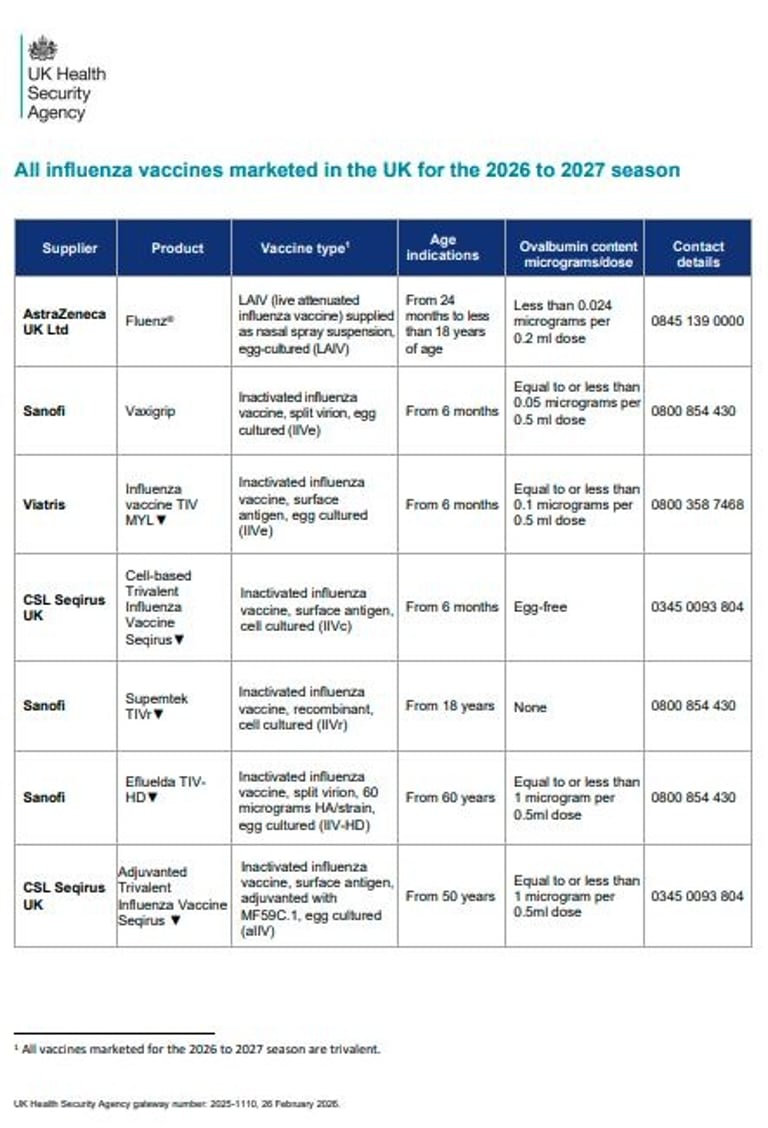
The 26/27 flu letter arrived 26/2/26. An amendment arrived 10/06/26. New eligible cohort: People experiencing homelessness. The Green Book chapter has been updated to reflect that people experiencing homelessness have been added to eligible risk groups. NHSE will issue further guidance on the addition of this cohort in due course.
We began the 25/26 vaccine clinics from 1st Sept for the kids and pregnant ladies, and 1st Oct for the adult and clinical risk groups 18+. 25/26 and 24/25 are the only years we have staggered the starts and this is due to quicker waning immunity in older adults than in youngsters. The rationale is that an extra month to wait means the vaccine protection will carry through to the end of flu season. 26/27 remains the same.
It's a massive undertaking to deliver the flu programme.
As of 23rd October 2025 we had vaccinated over 10.4 million (10,436,395) people against flu and almost three million (2,987,313) people against COVID. By 8th Jan 2026 over 18.6 million eligible people were vaccinated. BUT vaccine uptake across all groups has consistently dropped since lockdown times.
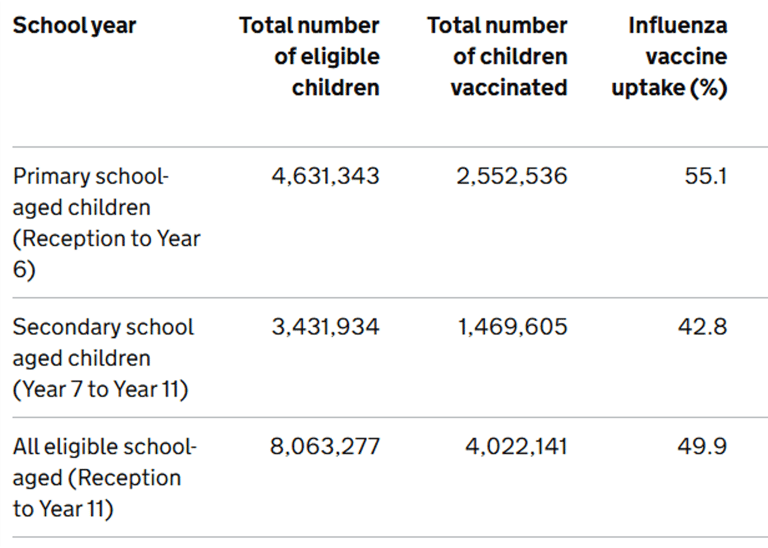
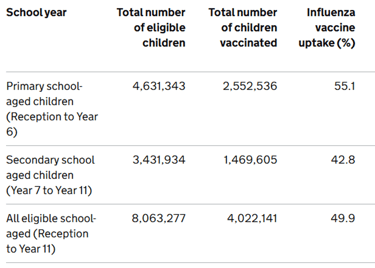
Where is this data from? Check out the GP patients uptake here and frontline healthcare workers here. Find the kids programme data here.
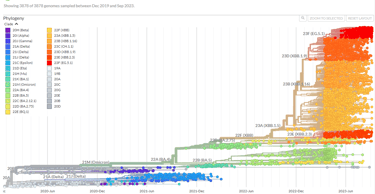
Why the need for boosters? New vaccines?Antigenic Drift and Shift: How the Influenza Virus Adapts









SARS COV-2 has changed a lot too. If you want to REALLY geek out try this website...
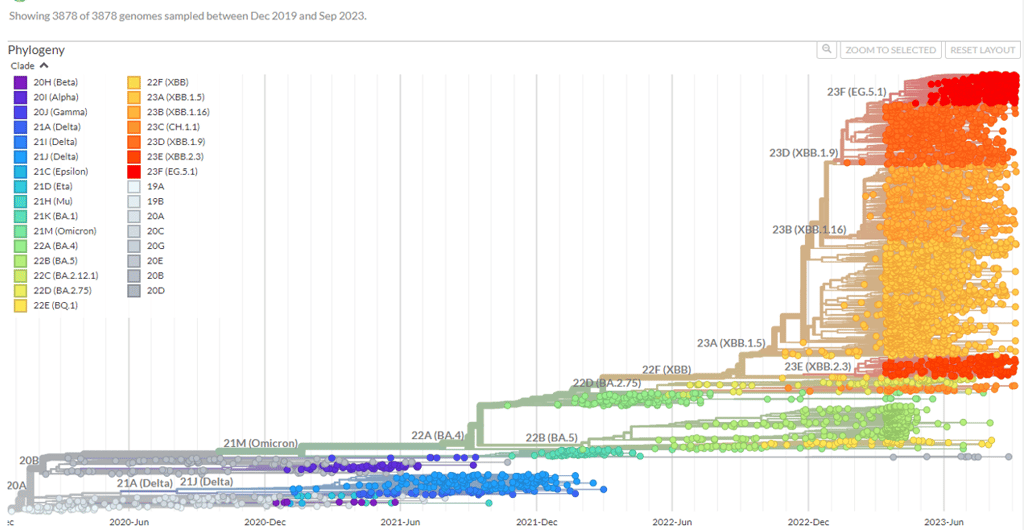

If you are particularly keen on the ins and outs of virus changes, also check out the section on SARS COV-2 epidemiology from the Green Book
Information on new variants under investigation is included in the weekly National flu and COVID-19 surveillance reports (if you are interested in this kind of thing!)
But back to flu. Let's take a closer look at the flu vaccines...

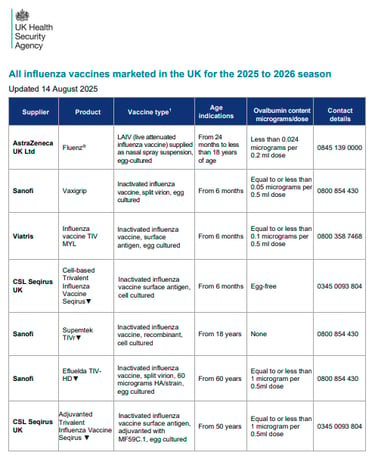
Ovalbumin content
LESS THAN 0.12MCG/ML = SAFE TO VACCINATE
(equivalent to <0.06mcg for 0.5ml dose)
Porcine Gelatine Content
Fluenz (nasal flu- LAIV) contains a small amount of highly purified porcine gelatine. This vaccine is the most effective option for children aged 2 and older but there is the (LESS effective) injectable alternative if required.
So, think carefully about how these conversations are had.... here's a blog with some practical tips for you.
Other queries about vaccine contents might be around microchips, dogs, sharks and moths...
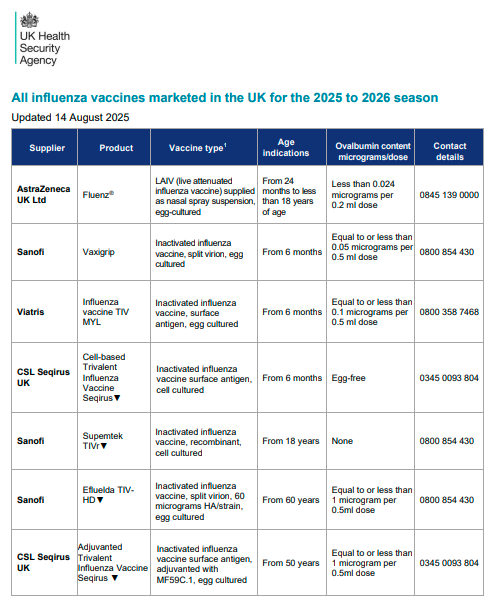
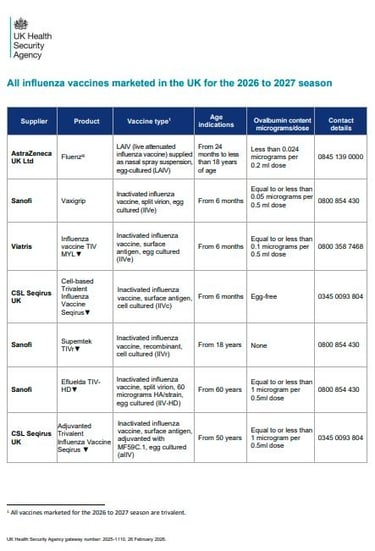
Quick tip: Note the little black triangles... When providing patients with details of the vaccine, it is good practice to give them details of the brand and batch number. This will allow patients and carers to more accurately report suspected ADRs to the Yellow Card scheme.
Quick bit of history: if you are new to this, you may still hear flu vaccines being referred to as 'QIV' (quadrivalent influenza vaccine) or 'TIV' (trivalent influenza vaccines) ... more seasoned flu vaccinators have had to change their terminology a lot over the years, so if a 'TIV' slips in instead of an 'IIV' on occasion - you know what it means!! The changes to terminology were about future-proofing consistency of language to avoid confusion down the line. Makes sense, but some us us feel that IIV doesn't quite roll off the tongue the same as TIV or QIV... politics eh? Learn more about what is meant by 'valency' in the video below.

Want to know more about vaccine production?
Sanofi (the first company to make a flu vaccine) made a video...
Watch it later if you fancy it.
QUICK CHANGES-FROM-LAST-YEAR NEWS! (if this is not your first rodeo)
Previous years have seen quadrivalent vaccines (4 strains) but 25/26 said goodbye to the Yamagata B strain (due to not circulating for a while) and all UK vaccines are now trivalent.
In 25/26 aIIV became licenced from 50 years
LAIV now includes PGD provision for up to 25y in SEN schools.
JCVI advise prioritising 2/3 year olds for 26/27. Community pharmacy got involved for the first time with child flu vaccinations in 25/26.
Community pharmacy service delivery for 2- and 3-year-olds will begin from 1 October 2026, supplementing the offer in general practice which will start vaccinating from the 1 September 2026.
Community pharmacy service delivery for children in clinical risks groups (from 2 years to less than 18 years) will begin from 1 October 2026, supplementing the offer by school-aged immunisation services (SAIS) providers, and in general practice and who will both start vaccinating from the 1 September 2026, or as soon as vaccine is available. NOTE: Children in clinical risk groups from 6 months to less than 2 years cannot be vaccinated by a community pharmacy.
Community pharmacy service delivery for school-aged children who missed the opportunity to be vaccinated by SAIS providers will begin from 1 December 2026
There are some firm words in the flu letter about planning to do more for uptake in 26/27, especially in under-served groups. The new GP contract aims to address these inequalities (and QOF) more fairly.
NHSE has now published the GP additional guidance for seasonal vaccinations 2026/27. This provides information on recording COVID-19 and influenza vaccination events and payments, including where practices are collaborating in their PCNs. In previous years this guidance has only covered the influenza programme. For 2026/27 it has been expanded to cover both the COVID-19 and influenza programmes.
There have been 2 changes to the JCVI advice for adult flu vaccines for 26/27. Firstly, in those aged 65 years and older, IIVc should be considered equivalent to allV, llV-HD, and IIVr. And secondly, in those aged 50 years to 59 years in clinical risk groups, IIV-HD can be used off-label (60+ licence).
NEW legal mechanisms! Goodbye to National Protocols and hello to the VGD! (and also the PGD has landed).

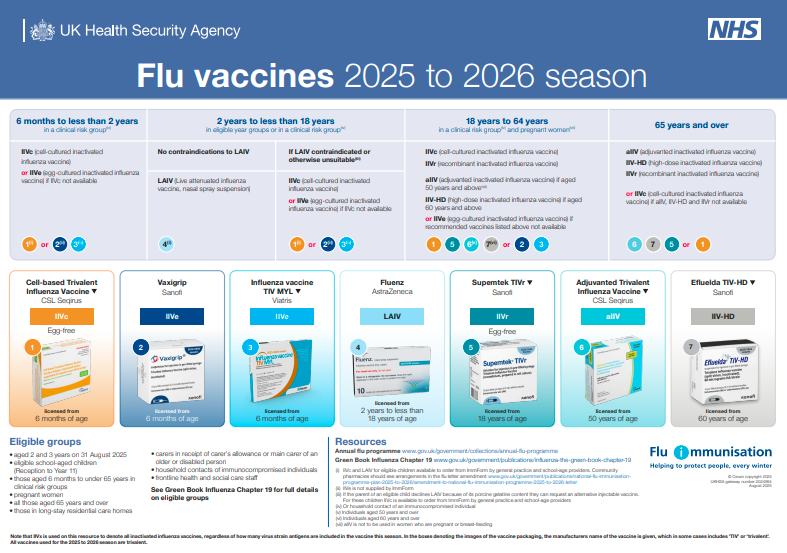
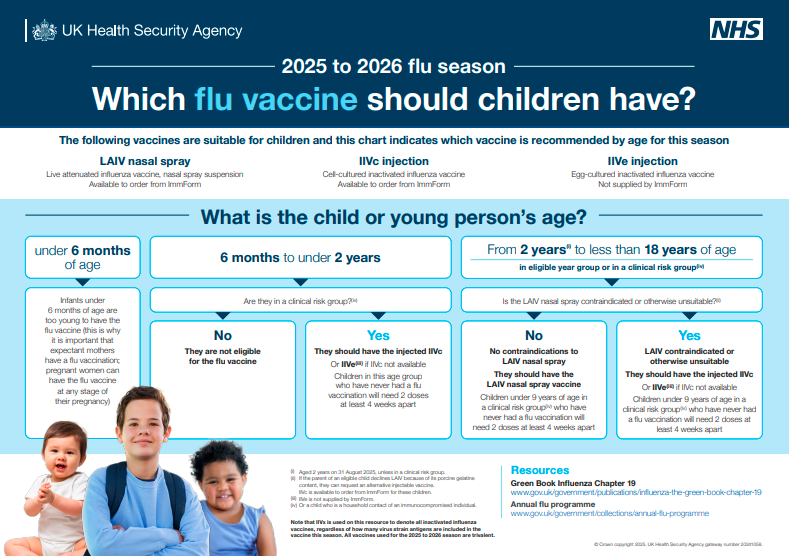
Keep an eye out for updated posters!

• LAIV is different from other flu vaccines – it is a live attenuated nasal vaccine and must not be injected
• Do not attempt to attach a needle
• Fluenz can be administered at the same time as, or at any interval from other vaccines including live vaccines
• Patient should breathe normally - no need to actively inhale or sniff
• The vaccine is rapidly absorbed so no need to repeat either half of dose if patient sneezes, blows their nose or their nose drips following administration
Administration of Nasal Flu Vaccine

IM administration
Note she doesn’t actually insert the needle in this demo (don’t forget to put it in!!!)


Results: "Access was NOT the primary issue underlying suboptimal vaccine uptake among participants in clinical risk groups, who instead cited low-risk perceptions of influenza infection and deficits of information about the relevance of vaccination for their condition management. Healthcare providers in non-primary care settings rarely discussed or recommended influenza vaccination across patient pathways, despite being able to address the concerns raised by participants in clinical risk groups." (I.E. vaccine uptake is not just about putting on the late night and weekend clinics! People may well make more efforts to show up if they knew WHY they should)




Flu vaccination in adult social care settings
Within the 99.1% of older adult care home providers who had updated their seasonal vaccination data as of 16 February 2026:
11.3% of total staff are known to have received a flu vaccination for the 2025 to 2026 season
66.7% of total residents are known to have received a flu vaccination for the 2025 to 2026 season
Within the 99.0% of younger adult care home providers who had updated their seasonal vaccination data as of 16 February 2026:
9.1% of total staff are known to have received a flu vaccination for the 2025 to 2026 season
54.5% of total residents are known to have received a flu vaccination for the 2025 to 2026 season
Reflection points (for ALL routine vaccines):
Do you know your local uptake figures?
In YOUR clinic, which are the most difficult groups to reach? Why?
Do you see similar results/patterns to the national figures?
What other vaccines might these groups be missing out on?
Do YOU have yours?

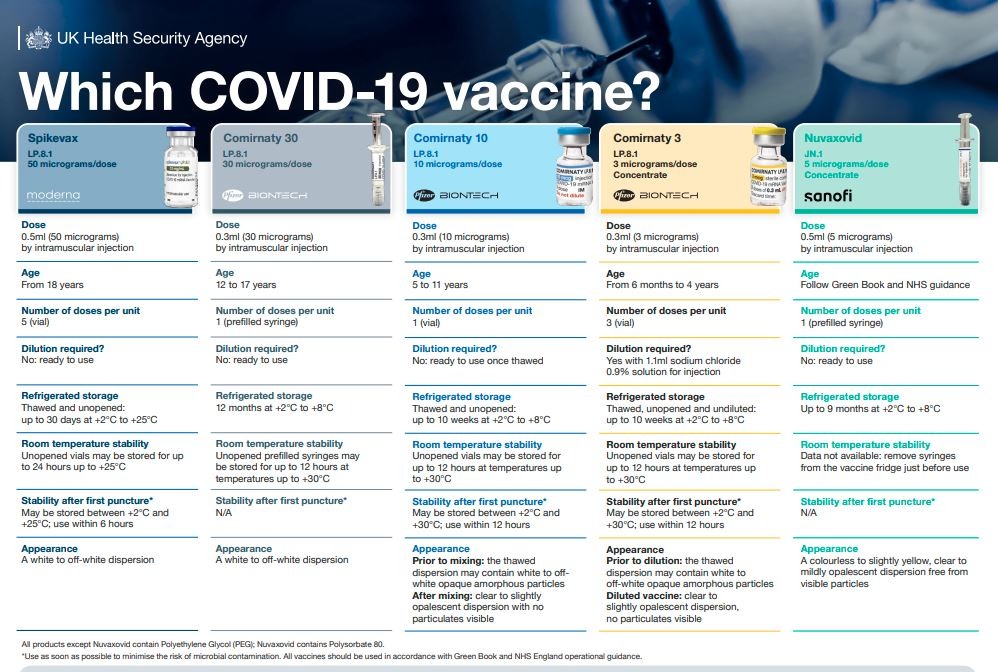
COVID-19
What a fabulous testament to vaccines and vaccine development: At least 15–20 million lives saved globally in the first year alone - and many more since - according to the modelling.
The primary aim of the national COVID-19 vaccination programme remains the prevention of severe illness (hospitalisations and deaths) arising from COVID-19, but, as the currently available COVID-19 vaccines provide only limited protection against mild and asymptomatic disease, the focus of the programme is now on offering vaccination to a more limited cohort who continue to be most vulnerable and are most likely to directly benefit from vaccination.
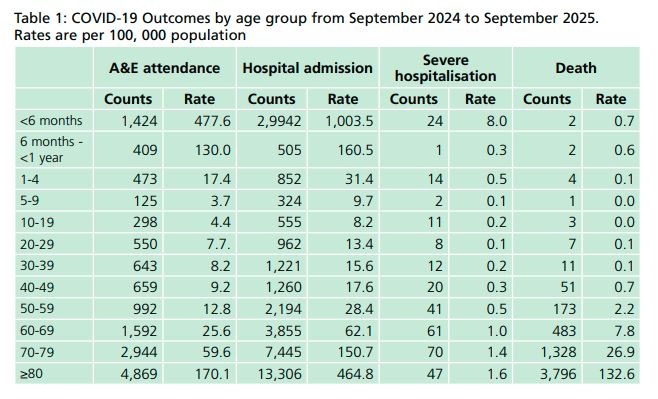
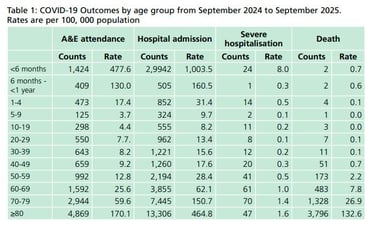
80% of deaths have been in those aged 70 years and over (check out the table below) and most of the excess all-cause mortality consisted of older age groups with more than 90% of excess deaths in those aged over 75 years.
Hence, eligibility is now 75+, care home residents, and IC 6m+.
COVID-19 vaccination is currently offered to eligible individuals twice a year, in Autumn and Spring campaigns (provided at least three months have passed since their last dose). Severely immunosuppressed individuals may be eligible for COVID-19 vaccination between campaigns. (JCVI considers that eligible children aged six months to four years of age should continue to receive two primary doses of vaccine).
Could COVID-19 move to an all year round prog? JCVI minutes from June 2025 indicate it's up for consideration.
The Autumn 2025 booster programme was 1st Oct-31st Jan. Spring vaccinations started on the 13th April and runs to 30th June - targeting high-risk groups only. All end-of-campaign actions are listed on the Vaccinations and screening Futures workspace. The year-round programme (for certain groups only) begins on Wednesday 1 July using Comirnaty, with vaccine requested via ICBs. Following JCVI advice, the autumn/winter 2026 COVID-19 vaccination programme will run (alongside flu) from 1 October 2026 to 31 January 2027.
Check out the latest variant vaccines (using the helpful poster below). Plenty of ongoing research. Hundreds of vaccines in development and vaccines are evolving – bivalent options, new variants, ?boosters, nasal options? Combined vaccines? Where is the 2 in 1 COVID and flu jab up to? Could this be with us in 2026?

Useful videos & resources for further learning

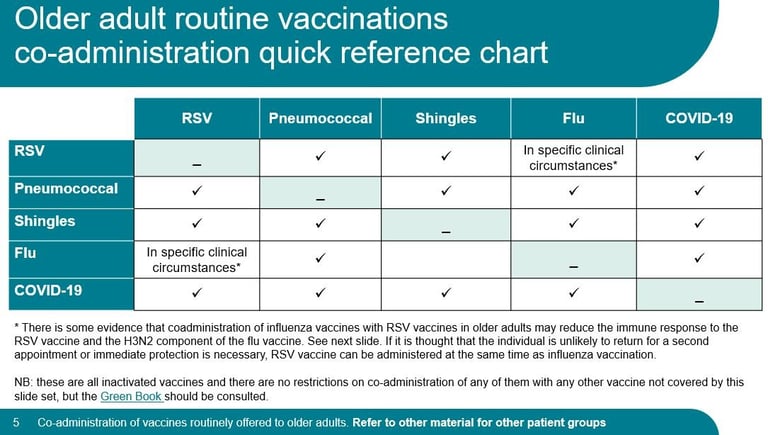
Giving more vaccines?
Click here for a useful UKHSA slideset about co-administration of adult vaccines from April 2026 (scroll down about a third of page to the heading 'Routine immunisation schedules')
Keeping up with changes & training standards: Here are your key resources:
National minimum standards and core curriculum for vaccination training. For all healthcare staff with a role in delivering vaccination programmes (June 2025)
The COVID-19 Green Book Chapter has now been updated and simplified (March 18th 2026). Check it out! Here is the Flu Chapter too (updated 14th May 2026).
PGD and VGD (note: NEW legal mechanisms! Goodbye to National Protocols and hello to the VGD!)
Find campaign resources HERE and HERE. And check out the hesitancy and uptake page on alyssclassroom.co.uk for more ideas for promoting vaccines.
Visit the news pages and vaccine portals for frequent updates on alyssclassroom.co.uk
And don't forget! Pandemic disruption has left much catching up to do with other vaccines.


Steve's Story.
Steve is 77
When he was 73 he developed meningitis and was hospitalised and in ICU for 7 days
Very nearly died. Long term sequalae since
Cause: Pneumococcal bacteria
Knowledge check: Do you know when he would become eligible for the pneumococcal vaccine on the NHS?
FINALLY given it age 75 (with Shingles vaccine – also late)
Multiple opportunities missed. Had EVERY COVID AND FLU VACCINE OFFERED. Never invited for the others. No-one noticed the other missing vaccines.
And it gets worse…. After the hospital admission, TTO on discharge accidentally missed out Candesartan. 7 days without it (absolutely no medical consequence though in this case).
Hospital realised. Incident form done, apology letter sent to Steve, phonecalls from Dr to apologise etc etc. But not a single mention of the missed pneumococcal vaccine (which COULD have led to the admission in the first place).
Why do we not take missed (or declined) vaccines as seriously when people can suffer and die from those diseases without them? Vaccines are important preventative MEDICINES too that people are eligible for and ENTITLED to – not without good reason! Whatever your scope of practice, learn to spot and highlight missing vaccines! Whatever vaccines you are giving you will automatically be seen as an authority on vaccines. Big responsibility.
Keep up the awesome work!!